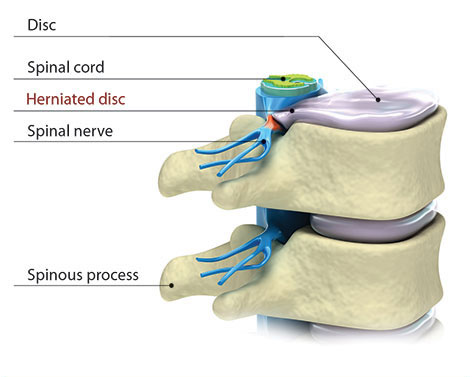
Learn about the shock-absorbing discs that separate the bones in the spine.
NOTICE: Our main Austin clinic location has moved to 1004 West 32nd Street. Click here for a map.
When children have spinal curves, physicians move cautiously. But now new research may be saying that waiting is not the best policy for children with spinal curves because they can quickly worsen to the point that more invasive surgery is required to correct the curve.
In the Canadian nationalized health care system, stories about patients having to wait many months for diagnostic studies and non-emergency surgeries are commonplace. These long waits for treatment represent the downside of government health care plans in Canada and the United Kingdom. Interesting researchers from Canada documented that long waits for treatment have shown to adversely affect the care of children in Canada who have scoliosis.
Researchers reported results from two studies about scoliosis treatment in a recent Canadian Medical Association Journal that revealed teens with scoliosis that wait more than three months for scoliosis surgery, risk further complications to their spine. Scoliosis surgery is one of the most common procedures performed in pediatric orthopedics.
The study found that patients waiting extended periods of time for surgery might need more surgery than originally to achieve the same results. Waiting for surgery can allow the spine to develop a worse curvature, which may require more blood loss and risk of damage to nerves (paralysis) when surgery is finally performed.
The study showed that waiting for surgery in patients that were skeletally immature or had larger curvatures of the spine showed the most adverse events for waiting for surgery. The researchers concluded that the younger the patient (teenage years) and the more they are in a growth spurt, the more risk that a spinal curve can quickly worsen.
The scoliosis research advised scoliosis surgeons to wait no longer than three months before acting, not the recommended waiting time of up to six months. The study showed that waiting longer than 6 months, 10-15% needed additional surgery that did not need at first, compared to 1.6% needed additional surgery who waited less than six months. Patients who waited longer also had longer surgeries and longer hospital stays.
For patients in the United States, this research implies that parents need to move quickly if they suspect their child has a spinal curve, and to be decisive when it comes to treatment, especially if surgery is recommended.
For more information on this research study, click to:
https://www.cbc.ca/news/health/story/2011/05/02/scoliosis-pediatric-surgery-wait-times.html
When scoliosis is present before the age of 3, this is known as Infantile Scoliosis. When scoliosis is diagnosed between the ages of 3 to 10, this is known as Juvenile Scoliosis. Children younger than 10 have special needs in scoliosis care.
Whether the cause of the scoliosis is infantile, juvenile idiopathic, congenital, from a connective tissue disorder, neuromuscular, or syndromic, the need for additional spine and rib cage growth to maximize eventual lung function is paramount. Techniques such as growing rods, titanium ribs (VEPTR, vertical expandable titanium rib), or growth modulating procedures (Shilla), are all options to maintain spinal and thoracic growth in young children with spinal deformities. It is important to involve a fellowship-trained spine physician that specializes in spinal disorders, such as scoliosis. Click here to learn more about Dr. Geck at Texas Spine and Scoliosis in Austin, he is fellowship-trained in adult and pediatric spine surgery.
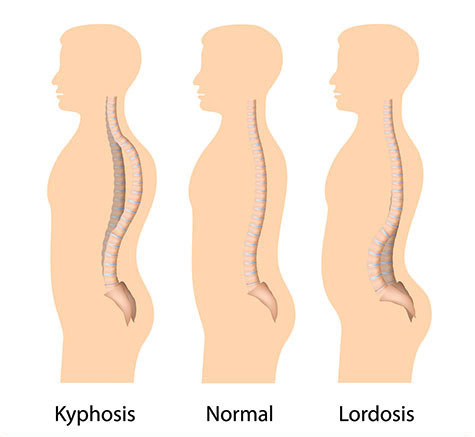
Congenital scoliosis is a condition where there is deformity in the spine present at birth, but will usually only be discovered as the baby continues to grow. Some of the reasons causing this type of scoliosis are abnormally shaped or fused bones in the spine that do not grow or fuse correctly. Kyphosis can be prominent here as well. Treatment should be individualized based on defects present and remaining growth. Emphasis here is to leave defects alone that do not need surgery, and to treat defects early that have large deformity potential.
Neuromuscular scoliosis consists of poor neurologic or muscular control of the spine and might be evident in a child born with cerebral palsy, myelodysplasia or Duchenne’s muscular dystrophy. Children diagnosed with more advanced scoliosis can often feel like they sometimes have trouble breathing and experience back/leg pain among other issues. Treatment should be individualized to maximize function and activity.
Most kids with non-severe scoliosis will not experience the painful symptoms that are often associated with scoliosis. Kids will usually be diagnosed either at a school screening being performed on the entire grade or by their doctor. Children with detectable scoliosis can appear to have a hump, “S” shaped curve in their spine, and perhaps uneven shoulders and hips while doing the Adams Forward Bending test. School examiners will inform the parent if they believe scoliosis might be present or could develop in their child. If scoliosis is discovered, it is important to see a scoliosis specialists to better evaluate the child and the doctor might take an X-ray for a better analysis. On an X-ray, the doctor uses the Cobb angle method to measure the angulations between the curving of the vertebrae.
The potential for the curvature in the spine to worsen correlates with the amount of growth remaining in the bones and spine. The amount of growth the child has left to complete is directly related to the amount and type of treatment he or she will receive since the ‘growth spurt’ years tends to make the scoliosis worse. One of the ways to measure how much growth the patient has left to complete is by taking a radiographic measure of the maturity of the pelvic bone. The Risser sign can be tracked on the pelvic X-ray to better determine if the person has more growing left to complete. The changes of puberty in girls and boys can also give insight if the person has more growing left as well. In girls, evidence suggests that the beginning of the menstrual period estimates 1.5 to 2 years of spine growth remain.
Bracing is designed to apply pressure to the trunk and pelvis, which improves the alignment of the spine and allows the spine to grow in a straighter fashion. Some doctors might recommend bracing if the scoliosis starts to pass 20 degrees measured laterally in the curve. Most doctors will recommend bracing for patients with a curvature angle around 20-50 degrees. Bracing is not designed to reverse the curvature, but rather to prevent the spine from increasing the angle of the curve. They are many different types of bracing options available with specially placed padding and straps that place resistance on the certain area in the spine. Most braces are constructed of plastic and contoured to your unique body and your doctor will help prescribe which brace is best for your treatment.
The Boston Brace is probably the most common used to treat scoliosis. These braces are made out of plastic components that are custom modeled to the patients body which creates a low-profile for the brace. On the front side, this brace extends from the lower breast to the start of the pelvic area. On the back side it extends from the upper back to the tail bone. This brace forces the lower back to flex which pushes the abdomen and helps flatten the curvature in the spine.
Although surgery can be risky and expensive, it might be an avenue to consider if severe scoliosis develops with a degree angle above 40 degrees and bracing has shown no signs of stopping the spine from continually to curve.
Children that don’t need bracing or surgery will still need to be under observation from the doctor to be aware if the spine continues to curve. The child will most likely be advised to come back for a couple follow up visits to make sure the scoliosis is not progressing into a serve curve. X-rays might be done semi-annually to make sure the curve does not worsen. Most of the time X-rays are conducted until the child stops growing or until the curving of the spine stops.
The majority of children diagnosed with scoliosis will not need any type of treatment. Less than 15% of children and adolescents diagnosed with some degree of scoliosis will actually need to begin some type of treatment including bracing and/or surgery.
There are not any specialized exercises that have been proven to help stop scoliosis. Most scoliosis in children should not prevent them from enjoying time with friends or playing sports.
 |
|
Click here to download |
Click here to download |