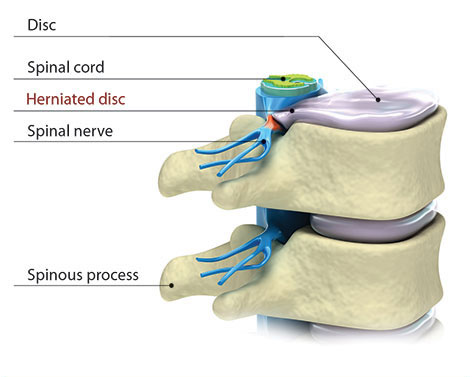
Learn about the shock-absorbing discs that separate the bones in the spine.
![]()
Types of spinal tumors | About treatment for spinal tumors
The neuro-spine physicians, Dr. John Stokes and Dr. Eeric Truumees at Texas Spine and Scoliosis in Texas are experienced in caring for and diagnosing a wide range of spinal tumors (neoplasia). Dr. Stokes is an expert in caring for primary spinal cord tumors, also known as intradural tumors.
 Dr. Eeric Truumees is experienced diagnosing and caring for primary and metastatic tumors from the occipito-cervical junction to the sacrum.
He has been published in this area, including an article in the Journal of the American Academy of Orthopaedic Surgeons entitled "Preoperative Embolization in the
Treatment of Spinal Metastasis" and chapters in several textbooks, including Rob McLain’s Cancer in the Spine.
Surgery for spinal tumors continues to evolve and the surgeons at Texas Spine and Scoliosis in Texas are at the forefront of the latest techniques and approaches for spine tumor treatment, both nonsurgical and surgical. The spine tumor treatment approach used by Dr. Stokes and Dr. Truumees works in association with medical and radiation oncology.
Dr. Eeric Truumees is experienced diagnosing and caring for primary and metastatic tumors from the occipito-cervical junction to the sacrum.
He has been published in this area, including an article in the Journal of the American Academy of Orthopaedic Surgeons entitled "Preoperative Embolization in the
Treatment of Spinal Metastasis" and chapters in several textbooks, including Rob McLain’s Cancer in the Spine.
Surgery for spinal tumors continues to evolve and the surgeons at Texas Spine and Scoliosis in Texas are at the forefront of the latest techniques and approaches for spine tumor treatment, both nonsurgical and surgical. The spine tumor treatment approach used by Dr. Stokes and Dr. Truumees works in association with medical and radiation oncology.
It is important for the orthopedic surgeon to have a complete medical history of the patient. This includes, understanding the prognosis of the patient, other areas of the body where cancer has spread and how the patient has responded to previous treatment. It is also important that the orthopedic surgeon have communication with the neuroradiologist.

Tumors that originate in the brain or spinal cord are called primary tumors. Primary tumors are extremely rare and slow growing. They occur in the vertebral column and develop from the bone or disc elements of the spine. Primary tumors more often occur in younger adults. The most common malignant bone tumor is the osteogenic sarcoma or osteosarcoma.
Primary bone tumors in the spine are very rare. The majority of spinal tumors are metastases. Of the sarcomas (meaning cancer of the bone, cartilage, fat, muscle, blood vessels, or other connective tissue) found in the body only 10% occur in the spine. CDC US Cancer statistics taken from the 2000 incidence report show the occurance to be between 2.5% and 8.5% per 100,000 people.
The more common type of spinal tumor is the metastatic tumor. The most common site of bony metastasis is the spine, nearly 20,000 new cases develop per year.1 Metastatic tumors occur when cancer spreads from another area of the body. Women more often develop metastatic spinal tumors from cancer originating in the breast or lung. While men are more likely to develop a spinal tumor from cancer originating in the prostate or lung. Symptoms of metastatic tumors include pain that does not get better with rest and may be worse at night. These symptoms may be accompanied by other signs of serious illness, including weight loss, fever or chills, nausea or vomiting.
New developments in oncology have resulted in cancer patients living longer. In turn, there has been an increase of metastatic tumors which cause pain, spinal fractures, spinal cord compression and other instabilities. Surgery may be necessary in some cases to help manage the pain and restore function. Nearly two thirds of the lesions that develop are often hypervascular, meaning a large number of blood vessels are present. The risk for life-threatening hemorrhage during the open surgery is increased because of this.
These are tumors that occur in the spinal canal, below the membrane that covers the spinal cord. These spinal tumors occur outside of the nerves. Intradural-Extramedullary tumors are non-malignant and slow growing. They may cause pain symptoms and weakness. The majority of intradural - extramedullary tumors are either meningiomas or nerve sheath tumors.
These are spinal tumors that occur in the membranes surrounding the spinal cord. Meningiomas are typically benign but may be malignant. They are more common in middle age and elderly women.

Spinal tumors (schwannomas and neurofibromas) that develop from the nerve roots that come off the spinal cord are known as nerve sheath tumors. This type of tumor is commonly benign and slow to spread. It may be years before a neurological problem occurs.
These tumors grow from inside the spinal cord or inside the individual nerves. They occur from the cells that provide physical support and insulation for the nervous system also known as glial cells. They are more often to occur in the cervical spine or neck. Intramedullary tumors are usually benign, though surgery to remove the tumor is complex. Intramedullary tumors are most commonly either astrocytomas or ependymomas.
Beyond surgical modalities, patients with radicular pain due to compression fractures that involve a tumor may benefit from nerve root blocks or other injection therapies.
Items to consider when selecting a treatment plan for spinal tumors include:
It is important for the orthopedic surgeon to have a complete medical history of the patient. This includes, understanding the prognosis of the patient, other areas of the body where cancer has spread and how the patient has responded to previous treatment. It is also important that the orthopaedic surgeon have communication with the neuroradiologist.
The surgeons at Texas Spine and Scoliosis in Austin, Texas have improved models for understanding the destabilizing effects of spine metastases. This allows them to take preventative action in stabilizing patients at risk for catastrophic spinal column failures. This makes for better pain control, return to function and medical management.
Surgical options range from percutaneous biopsies and cement stabilization to wide resections of primary malignancies. Hybrid, mini-open and less invasive screw and rod stabilization modalities have evolved rapidly as well. Thus, a needs based treatment strategy can be selected that recognizes the patient’s short and long term goals.
Treatment decisions in patients with spinal metastases are complex. The surgeon and patient will work together to develop the best treatment plan for each individual patient.
The usual goal of surgery to remove a spinal tumor is to protect the spinal cord and to control pain. The surgery does not often affect the overall course of the disease. Because nearly two thirds of the lesions that develop are hypervascular, meaning a large number of blood vessels are present. The risk for life-threatening hemorrhage during surgery to stabilize a spine tumor is increased because of this.

A preoperative angiographic assessment is advised for any patient undergoing open stabilization of a spinal tumor. When the angiogram identifies hypervascularity, embolization may be used. Pre-operative embolization is a technique used to obstruct the blood vessels that feed the tumor. Embolization may be used for patients of all ages. For some benign tumors, embolization may be used in younger patients to delay surgery until they are older. Other advantages of embolization include: decreased blood loss during surgery, improved visibility during surgery and reduced surgery duration. In some cases, embolization may decrease tumor recurrence.
Alternatives to embolization focus on various pre- and intraoperative maneuvers to decrease lesion vascularity or achieve hemostasis. In some cases, neo-adjuvant radiation therapy (XRT) or chemotherapy may help to reduce the size of spinal metastases. A reduction in metabolic activity in the tumor may help to reduce vascularity. It is important to note that preoperative XRT is associated with a higher level of post-op wound complications than embolization. Bleeding can be also be lessened by injecting small amounts of sterile alcohol directly into the lesion.2
Sources:
1. Gokaslan ZL: Spine surgery for cancer.
Curr Opin Oncol 1996;8(3):178-181.
2. "Preoperative Embolization in the Treatment of Spinal Metastasis"
Truumees et al. J Am Acad Orthop Surg.2010; 18: 449-453
[top]